Exploring the frontiers of Herbal Medicine for the 21st century and applying Integral Theory to the development of an Integral Herbal Medicine and an Integral approach to Health and Wellness.
Well, anyone who has studied the effectiveness of natural immunity post-infection by COVID-19 or has a good understanding of immune function in general could have told you this. There have been numerous published studies showing little to no benefit of vaccination on-top of natural immunity. But here is yet another study which looks specifically at the 4th “booster”. Now there may be plenty of people who refused vaccination, or were not privileged enough to access vaccination and there are even fewer hermits out there who have not yet had COVID so the implications of this paper are far-reaching. And easily summarised – boosters are of no use (and carry significant potential for adverse impacts known and un-known) except for boosting the profits of one of the worlds most rapacious industries.
Well, herbalists would agree with this conclusion wholeheartedly. I’m sure there are methodological limitations to this study but the core principle is solid: better nutrition (food and supplements) will reduce the burden of chronic disease both financially and in terms of suffering. The pharmaceutical model of health care fails drastically when it comes to addressing chronic disease (the proof is in the name chronic) and the cost of often ineffectiveness medications taken for decades that do even if they do have some effect rarely alter the disease process is also dramatic. The limitations of the pharmaceutical model is illustrated by the financial costs of the impact of chronic disease under the status quo. So….why aren’t insurance companies and medical institutions encouraging a lifestyle, nutritional, and natural supplement and herb approach????
Many herbalists would say that one needs to use NSAIDs with caution because they interfere with the inflammatory process. Think about it…inflammation is one of the many functions of the immune system and has evolved over millions of years as an effective response to injury. Pain and inflammation prevent over-use of the injured body part (thereby reducing chance of further injury), provide immobilisation, and begin the process of healing via the recruitment of immune cells and an increase in circulation. So shouldn’t this process be enhanced rather than suppressed? Can pain be reduced without interfering with the healing process? It would seem that many NSAIDS may interfere with the process of healing, as demonstrated by this study, thereby resulting in an increase in chronic pain. When I broke my clavicle on a martial arts accident a few years ago I read that NSAID interfere with the chondrocytes that are recruited to help repair the bone. So I skipped the offered pain killer (I took one paracetamol in the emergency room and that was it) and instead used a herbal cocktail. In herbal medicine we talk about immunomodulators instead of anti-inflammatories. Curcumin and boswellia are prime examples – they do not interfere with the inflammatory process, yet they reduce inflammation, and pain, while actually promoting circulation and healing. They optimise the inflammatory response while preventing it from entering into the vicious cycle so common in chronic pain conditions. As a result my cocktails of herbs the nurses were surprised at how little inflammation I had and how little pain I was in. So next time you experience an injury consider using herbal medicine to modulate the inflammation, promote healing, improve circulation, and reduce pain. You can optimise your chance of full recovery and minimise your chance of developing a chronic condition. Its worth noting that herbalists take a similar perspective in regards to infections and the accompanying immune response (especially fevers) and that an inadequate immune response (due to deficient immune function or to use of drugs such as paracetamol) may increase the chance of developing post-viral syndrome (or “long COVID”).
Short-term use of ibuprofen may increase chance of chronic pain, study suggests | Health | The Guardian
It speaks for itself but who will hear it? Yes another unambiguous study showing the direct correlation between low vitamin D levels and severe infection/mortality with COVID and conversely the reduction in risk as vitamin D levels improve. The failure of public health organisation around the world to promote vitamin D is one of the gravest failings of the “pandemic” response and frankly the medical establishment should be ashamed for failing to follow through with the evidence.
Based on data from France the authors found that mortality rate from the Astra-Zeneca vaccine was higher in younger age groups than mortality from COVID infection. This study uses data from before Omnicron which would reduce the COVID mortality numbers. Similar finding have been seen in Norway, Denmark and the UK. The results and a conclusion are quoted below and they speak for themselves. I’m not sure how any health practitioner could recommend a vaccine to an individual where the mortality rate from the vaccine is higher than the infection it purports to protect them from! This is yet another study pointing towards the need for a very nuanced vaccine strategy that only targets those with risk factors.
Eurosurveillance | Benefits and risks associated with different uses of the COVID-19 vaccine Vaxzevria: a modelling study, France, May to September 2021
“In all distribution strategies, the number of COVID-19 deaths averted with the use of Vaxzevria in individuals 55 years and older was substantially higher than the expected number of deaths from TTS in that age group. For instance, using Vaxzevria in those 55 years and older would avert 355 deaths in this group while causing three deaths from TTS”.
“When Vaxzevria was used in younger age groups, the benefit–risk balance was no longer as favourable and even reversed in the younger age groups. For instance, using Vaxzevria in the entire adult population would avert four COVID-19 deaths in the 18–29 year-olds and six in the 30–39 year-olds, but it would be associated with 12 and nine deaths from TTS in these age groups, respectively.
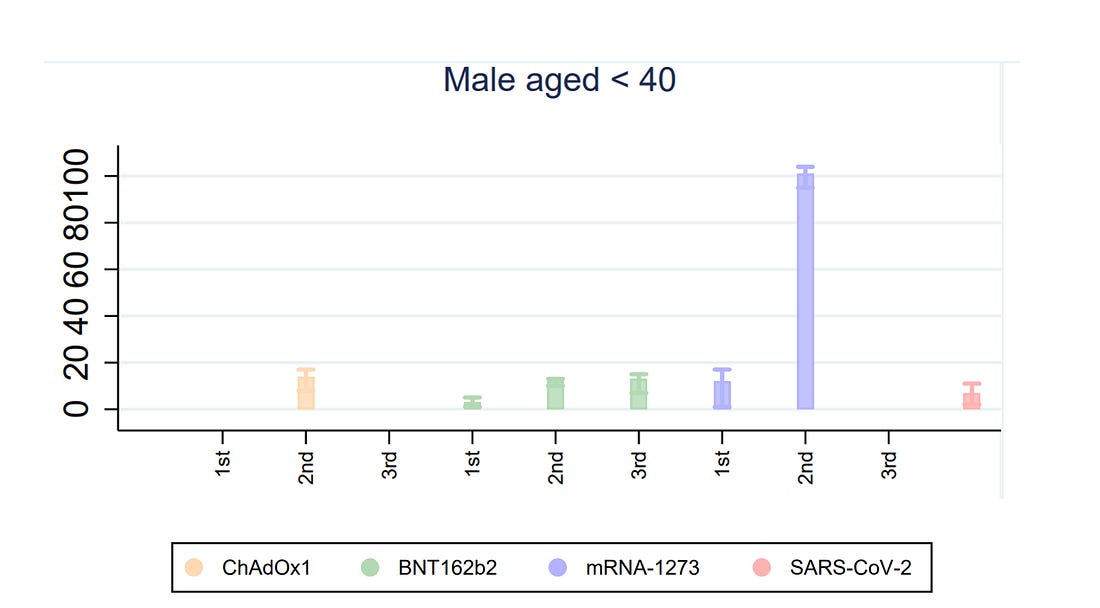
One of the arguments used against those wishing to avoid vaccination is that COVID is more likely to cause myocarditis than the vaccines. This assertion was not backed with sufficient data at the time and now there is strong evidence that it is patently false. The risk of myocarditis is greater from vaccines, especially in young men and in particular with the second dose of Moderna as well as from Pfizer.
Here’s a bit about Myocarditis from the Mayo Clinic in my home state of Minnesota.
“Myocarditis is an inflammation of the heart muscle (myocardium). The inflammation can reduce the heart’s ability to pump and cause rapid or irregular heart rhythms (arrhythmias).
Myocarditis is usually caused by infection with a virus. Sometimes myocarditis can result from a reaction to a drug or be part of a more general inflammatory condition. Signs and symptoms of myocarditis include chest pain, fatigue, shortness of breath, and rapid or irregular heartbeats.
Severe myocarditis weakens the heart so that the rest of the body doesn’t get enough blood. Clots can form in the heart, leading to a stroke or heart attack.”
This is followed by a more complete list of symptoms for adults and children.
Now lets get into some current publications on the subject.
Study 1:
“Risk of Myopericarditis following COVID-19 mRNA vaccination in a Large Integrated Health System: A Comparison of Completeness and Timeliness of Two Methods”
This study was conducted in the US using data from the Kaiser insurance company and the author made an effort to search out cases that had been missed by the VAERS passive reporting system (the equivalent in the UK is the Yellow Card).
Lets take a look at the risk of vaccine-induced myocarditis for 18-24 after the first dose 252/million (male and female) and for second dose 537/million (male only) or 1/1862 will experience myocarditis according to this study. These align with results published in a separate study in Nature as well as with data from several countries.
Study 2 compares risk of myocarditis from vaccination versus COVID:
Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection
(ChAdOx1 is AstraZeneca, BNT162b2 is Pfizer, mRNA-1273 is Moderna)
This study, conducted in the UK, had very similar outcomes with rates of vaccine induced myocarditis for both Pfizer and Moderna higher than from COVID for the first dose with a dramatic rise for the second dose. Studies from other countries confirm that Moderna comes with a higher risk of Myocarditis compared to Pfizer. We need to keep in mind that these studies both have some inherent limitations:
1 – Because many COVID infections go undiagnosed due to being asymptomatic/untested, the ratio of myocarditis/million of infections is inflated, and thus the risk of myocarditis will be over-reported.
2 – Under-reporting of vaccine-induced myocarditis. In general it is known that adverse reactions to drugs are significantly under-reported. The Kaiser study takes measures to count cases that were not reported by the standard VAERS procedure (a reporting system for adverse drug reactions). However both studies are likely to miss out on some adverse reactions. Let’s think psychologically for a moment and do a bit if stereotyping…what age group and gender are most likely to ignore their physical health condition? Probably exactly the group that is at the highest risk in this case ‘healthy young men’.
A third study conducted using health data in Canada comes to a similar conclusion. The author advises using vaccines carefully, especially in the population for which COVID risk is low and vaccine induced myocarditis is high. For example, limiting the vaccine to a single dose, or avoiding vaccines linked to higher chances of myocarditis.
Study 3:
Epidemiology of myocarditis and pericarditis following mRNA vaccines in Ontario, Canada: by vaccine product, schedule and interval
Contextualising the Risk and Benefit within a medical and ethical framework.
So lets take a deeper look at risk-benefit of vaccines in light of this new research and taking into account the decreasing severity of COVID due the Omnicron variant displacing previous variants.
To get an idea of the risk-benefit balance of vaccination, we need to take a look at mortality figures by age group by clicking on the ONS link below for UK data. As you can see mortality from COVID in the 20-24 age bracket is very very low, however risk of Myocarditis contracted from the vaccine in that same bracket is considerable…
Keep in mind that the mortality rate from COVID will plummet with Omnicron which is far less severe. Probably the infection induced myocarditis will also plummet.
However, the vaccine-induced risk, which is under-estimated will remain consistent, though it may increase or decrease with further doses. The risk of vaccine induced myocarditis will remain significant with every so-called “booster,” even as the purported benefits of the boosters become less and less. So the risk-benefit balance will be dramatically altered.
“A Japanese bio-distribution study for the Pfizer vaccine found that, in the 48 hours post-vaccination, vaccine particles had travelled to various tissues throughout the body and did not stay at the injection site, with high concentrations found at the liver, bone marrow, and ovaries.”
If an auto-immune and inflammatory reaction is triggered at any of these sites there is a distinct possibility for long-term, initially sub-acute, adverse effects.
In a world with endemic COVID-19 everyone is likely to eventually get infected. For individuals who have a history of previous infection the temporary increase of antibodies given by the booster on top of natural immunity provides a few percentage benefit in decreasing infection but little to no benefit in regards to severe infection or mortality. Why? Because natural immunity provides, at least in this study 100% protection from severe illness. The study from Qatar showed that individuals with re-infection had ZERO severe infection or mortality, and that was pre-Omicron.
Severity of SARS-CoV-2 Reinfections as Compared with Primary Infections
If a study conducted outside the US isn’t good enough for you the CDC has finally published a properly conducted study looking at natural immunity (pre-dating omnicron). Same results: natural immunity beats vaccination hands down.
COVID-19 Cases and Hospitalizations by COVID-19 Vaccination Status and Previous COVID-19 Diagnosis — California and New York, May–November 2021
From an ethical and moral standpoint I question the strategy of imposing a risk of harm onto a large population of healthy individuals (low risk from infection) to ostensibly protect a small population of individuals (those at high risk from infection). Though the mortality rate from COVID is highly variable, largely due to the co-morbidities within a given population (which are much higher in the US and Europe than in developing countries but that’s another story) we see estimates such as 0.15%. Yes, this adds up to large numbers of deaths, but statistically speaking mortality rates are very low. Furthermore, context is important. In the case of a disease like small-pox, which is indiscriminate (i.e. we can’t predict who is high risk) and has a very high mortality rate (as high as 30%) there is possibly a much stronger argument for vaccination.
In regards to medical ethics an individual has a basic human right to determine the medical interventions that they are subject to, except in very limited circumstances. I do not personally think that COVID-19 ever met these criteria. Different folk will have a differing value-system in regards to this question. It is by no means a strictly objective process as measures taken against COVID must take into account the impact of both the measures themselves and of the virus as the situation (and our knowledge) evolves. In addition to this foundational principle there are five reasons, well-established by research, that further weaken the rationale for imposing vaccination en masse and shift the balance towards a more-nuanced strategy
1 – Vaccines effectively reduce mortality and severe disease in high-risk individuals. This is the important point. Vaccinated individuals are less likely to die from COVID.
2 – Vaccines do little to reduce transmission. Vaccinating a 20 year old man, who thereby has a 1/1862 chance of myocarditis along with other side-effects has a known risk but little benefit in regards to reducing transmission to others. There are now many studies demonstrating this.
3 – A fully vaccinated population still gets infected. We have highly vaccinated countries with large outbreaks (Israel, etc), and now we’ve had two US Navy ships and two cruise ships with 100% vaccination in addition to testing that have had outbreaks.
4 – The decreasing severity of new variants along with the decreasing ability of vaccines to prevent infection to new variants. There is no insurance that a new variant might “buck the trend” and have more severe symptoms. However this would be moving against the gravity well, so to speak, of the development of a stable relationship between host-virus. This is an established evolutionary pattern and all evidence points to it playing out with COVID-19 (as it did with the 1918 Influenza).
5 – In addition to vaccines we have many other interventions, both natural and pharmaceutical, for the treatment if COVID with the goal of preventing severe infection and mortality.
In light of these 5 points there appears to be little rational reason to impose vaccination (and potentially other measures) on our young and healthy population for the sake of our at risk-individuals. The CDC study, one amongst many, shows emphatically that vaccines for individuals with previous infection are not only unnecessary but contrary to the well-being of the individual while conferring no benefit in regards to the herd. In terms of boosters their need, especially in low-risk individuals, is also highly questionable. According to World Health Organisation chief scientist, Soumya Swaminatha; “There is no evidence right now that healthy children or healthy adolescents need boosters. No evidence at all,” (https://www.youtube.com/watch?v=oIa0hAimtfU). So it seems that the primary beneficiary of indiscriminate vaccination and continued boosters (given before the research supported their need!) is the pharmaceutical industry.
A Herbalist’s perspective
My mantra is “treat the risk factors” – ie take a both/and approach to the “Terrain” versus germ theory argument. This requires supporting the individuals’ resilience in a holistic fashion as well as addressing specific risk factors (diabetes, obesity, etc) and strengthening the immune system. Whether someone decides to vaccinate or not, this is simply a good idea both because it will reduce risk from COVID, improve the immune system’s response to the vaccine, promote overall good health, and reduce morbidity from many causes.
The other question is what to do for those who have had myocarditis as an adverse reaction? This is tricky as the mRNA vaccines are a trigger completely novel to life on Earth; the human species has simply never encountered them and so we don’t know exactly how and why they are triggering adverse reactions and have zero experience of how to treat those adverse effects beyond anti-inflammatories and assuming the body will take care of itself (which it will to a large extent). There is however no precedent and no long-term data as to whether, for example, the vaccine induced inflammation results in scar tissue on the heart or other consequences. My inclination would be to take a functional approach using heart-healthy herbs such as Crataegus, anti-inflammatories such as Curcumin, immuno-modulators such as Echinacea and adaptogens such as Ganoderma (Reishi), Withania, Eleutherococcus, etc. This would be in addition to an anti-inflammatory diet that is supportive of healthy vasculature. Such a diet looks something like this: healthy fats, low carb, very low sugar, loads of vegetables, and fruit (especially berries), fish, organic meat if desired. Such a diet has the added benefit of being the foundation for the treatment of many of the risk factors. This approach is likely to speed recovery from myocarditis while preventing the development of a longer-term auto-immune dysfunction and further damage to the heart.
Well this is a surprise, finally the CDC publishes a methodologically strong study (a rare event!) about natural immunity. Well, to be more specific comparing the protection gained from previous infection to that from vaccination, as well as to those who have vaccination followed by infection.
The results show that infection confers better protection against re-infection, and hospitalisation than vaccination alone. (Other studies around the world and in the US have shown this, including 100% effectiveness against severe illness and mortality but the CDC and US government have ignored them!). The study is from the Delta period and risk of infection will be significantly decreased with Omnicron (current UK figures show omnicron to result in about 1/2 the mortality of a bad flu season…so take it seriously but no need to panic!).
The study clearly shows that though vaccine protection wanes after a meager 3 months natural immunity remains strong.
So if you’ve already had one variant or another of COVID you can relax, you have lifelong protection from severe illness (most likely) whether or not you’ve been vaccinated. Vaccination will confer little to no extra benefit (but comes with increased risk of adverse events if you have had previous infection). With delta replacing omnicron I think we can assume most will soon have natural immunity and only those with co-morbidities need to consider, in consultation with health practitioners, whether vaccination is appropriate. Time to move away from one-size fits all medicine!
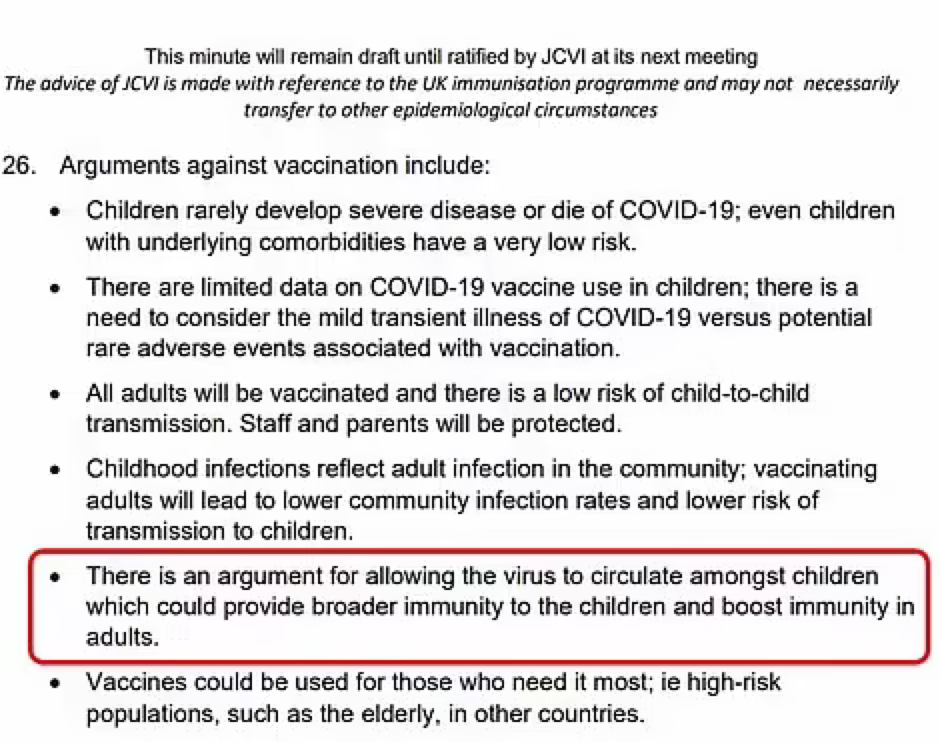
As we think about vaccinating children there are many considerations to take into account. The Joint Committee on Vaccination and Immunisation (JCVI) itself recommended against vaccines for the 12-15 age bracket considering that the risks outweighed the benefits. Now the US is pushing vaccines on children aged 5-11 and possibly even lower. As individuals consider the question of vaccinating their children, and as the UK might consider going down the same route, I thought it was important to bring together some research that sheds a different light on the matter.
Below is an excerpt from the minutes of a JCVI meeting held on 13 May ’21
In this piece I will address a few questions pertaining to the risk of COVID for children: why their immune systems handle it so well, the risk/benefit of vaccines (using Pfizer vaccine as an example) and the case against vaccinating children from both the individual and public health perspective.
Risk of Covid in children
“Between March 2020 and Feb 2021, 3105 people under 18 died in England and Wales. Among those were 25 deaths from Covid. Half of those children had underlying complex conditions with high health-care needs, such as tube feeding or assistance with breathing.”
There are 12 million children in England and Wales. Statistically this means that out of every 1 million children in England and Wales, 2 children died from Covid. Half of these will have complex healthcare needs and the other half likely have other co-morbidities such as obesity (Interestingly there has been a dramatic rise in childhood obesity during the various lockdowns. 1 in 7 children are now obese (https://www.dailymail.co.uk/news/article-10207641/Childhood-obesity-hits-record-high-Covid-NHS-data-shows.html). ).
So from a statistical perspective the risk of children dying of Covid is very low.
Why is the immune system of children so much more effective when it comes to COVID?
Several factors are likely contributing, including a stronger innate immune response (as opposed to the adaptive immune response that vaccines stimulate), less inflammation and fewer co-morbidities.
The JCVI states that “children might be better off catching COVID at a young age, when they are at low risk, so that they are less vulnerable in adulthood, as is the case with chicken pox and other viral infections” (minutes from JCVI meeting on May 13th 2021).
It is important to keep sight of this wider perspective and not give in to a knee-jerk reaction to the situation that provides us with a single solution (vaccines) at the expense of all other considerations. Such a reaction may result in significant collateral damage in the form of short and long-term adverse reactions (which have not yet been studied), and failure to address underlying risk-factors which impact on our general health and longevity. There are also huge socio-economic costs associated with the vaccine program.
Most importantly, the vaccine-only route may also fail to help us achieve our goal of minimising the suffering caused by COVID. The JCVI wishes to avoid the trap of overmedication, which we have fallen into so disastrously with antibiotics. There is great risk in taking a singular perspective and not allowing for a fuller, multi-perspectival approach.
The JCVI contextualises COVID within our knowledge of other viruses such as chicken pox. Taking a wider view when looking at our current situation by looking through evolutionary, and ecological lens allows us to better understand the natural course of an encounter between a virus and a new host. We need to understand how the relationship between the host and the virus moves through time (evolutionary) and space (ecologically). How this relationship evolves over time is largely mediated by the mutations of the virus (how it adapts to us) and our natural immune response (how we adapt to the virus). This progression that has occurred innumerable times since mammals and viruses first met millions of years ago involves viruses adapting to us by becoming more transmissible and less symptomatic and human immune systems recognizing the virus more swiftly and dealing with it efficiently without over-reacting. This process is inevitable, and we could be actively facilitating it (by supporting immune function for example) while protecting high-risk individuals (with vaccines, drugs, vitamin D and by addressing risk factors). Instead we have lost sight of the natural course of events and are engaging still with a warfare mentality.
Vaccine safety in children
Now let’s have a look at the specifics of the safety and efficacy of the vaccine when it comes to children. In doing this I am referring to US data drawn from Pfizer trials. As there have been no UK clinical trials. For the moment I will bracket the issue of Pfizer’s integrity when conducting clinical trials, which is highly suspect: (https://www.bmj.com/content/375/bmj.n2635 This is not an isolated incident; Pfizer has a long history of unethical marketing and even an illegal clinical trial conducted in Nigeria which resulted in the death of 11 children and disability to dozens.)
Below is a link to the data report from the trial their vaccine trial:
Since the beginning of the pandemic there have been 94 deaths in the US among children aged 5-11 with COVID having been diagnosed (though this does not necessarily mean the primary cause – it can be very hard to sort this out). There are 24.9 million children age 6-12 in the US in 2021 (https://www.childstats.gov/AMERICASCHILDREN/tables/pop1.asp). We don’t have a perfect age overlap but that gives us a rough indication that we might be looking at around 3-4 deaths from COVID per million. It’s worth noting that the US probably has the highest rate of childhood obesity in the world.
There are numerous issues with the trial:
Pfizer concluded that the trial was a big success. The vaccine is very effective at preventing infection and 100% effective at preventing death! But then so was the placebo: no children died with or without vaccines. Neither were any children hospitalized in either group. As we have already seen, mortality among children from Covid is exceedingly rare, and the very small sample size in this trial (1461 children in the vaccine group and 714 children in the control group) means that you cannot draw any valid statistical conclusions about effectiveness. Severe illness is unlikely to have shown up in such a small trial, vaccine or no vaccine.
With regards to adverse reactions, the trial shows a high rate of “normal” vaccine side-effects (sore arm and so on) but is not big enough for myocarditis, pericarditis, anaphylactic shock, blood clots, or other severe reactions, including death to show up. Nor was the trial conducted over a long enough period for long-term effects to show up.The typical Pfizer vaccine side-effects for adults are below:
For adults: Anaphylaxis 11.1/millions.
Bell’s palsy .2/1000 (Which is less 4x less than from infection).
Acute Myocarditis: 1:3000 to 1:6000 Men 16-24.
It’s worth remembering that adverse reactions to drugs are heavily under-reported. I’ve seen estimates that 5-10% of adverse reactions are reported. If children responded the same as adults then we can see quite a high number of individual children will experience severe side-effects.
Multiply the chances of severe adverse reactions by several times if the child has natural immunity. A study in the UK has found that individuals who previously had a Covid infection, ie with natural immunity, and are then vaccinated have a greatly increased risk of side-effects (for Pfizer specifically: 2-9x chance of side-effects and 56% increase in adverse reactions requiring hospitalisation). It’s important to remember that some side-effects may not show up for years or be contributors to more complex multi-factorial health problems.
Though myocarditis appears to resolve within a few months it’s important to note that there may be risk to other tissues in addition to inflammation of the heart and that the effects may not be immediately apparent. Newly published researched has shown that mRNA vaccines trigger elevation of inflammatory markers associated with an increased risk of ACS (Acute Coronary Sydrome). 5 Year risk of an ACS event (which includes hear-attacks) was raised from 11 to 25%. (https://www.ahajournals.org/doi/10.1161/circ.144.suppl_1.10712) We have no idea how long these markers, signs of inflammation, will remain elevated. Is this a risk we want to take with low-risk individuals, particularly our children?
Does it make sense to treat individuals for a health concern that is not problematic to them? The age group itself is negligibly impacted by COVID (first of all children tend to be barely symptomatic when they catch Covid, and secondly natural immunity provides much better protection against future variants of the virus). The vaccine is likely to cause a higher incidence of adverse reactions than Covid infection would, which counters the potential benefits of vaccination.
Should we really indiscriminately vaccinate a million children to protect 2-4 children? Does this make sense taking into account the unknown risks? What about protecting the vulnerable instead? I suggest this would provide great benefit at very low risk and cost.
The other argument made for vaccinating children is in regards to reducing transmission to potentially at-risk individuals. However, it is well established that vaccines don’t prevent infection or transmission. A study int he Lancet demonstrated that the transmission in a household was as likely from a vaccinated as from an unvaccinated individual. Wether vaccinated or unvaccinated, an infected child will potentially transmit within their household. (https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(21)00648-4/fulltext)
In either case they are likely to be asymptomatic. A child (or adult) with natural immunity will be more likely to “break the chain” of transmission with no need to account for immunity waning within as little as 3 months of vaccination.
Addressing the risk factors:
How about addressing the risk factors? Can we be bothered? Neither the media, nor the government, nor even the scientific journals do justice to this strategy. A striking example is vitamin D3 deficiency. A recent meta-analysis shows that a mortality rate close to zero could theoretically be achieved with adequate vitamin D levels. Such an intervention would have minimal cost and nearly zero risk, along with multiple side benefits, as low vitamin D3 is implicated in many health conditions. (https://www.mdpi.com/2072-6643/13/10/3596).
I have already mentioned the pandemic of childhood obesity and diabetes. Both of these are risk factors not just for COVID but for many other causes of mortality including heart disease and cancer.
Treating obesity and diabetes would dramatically reduce morbidity and mortality over the course of the lifetime with the added benefit of protection from COVID.
Obesity related illness costs the NHS 6 billion pounds per year. The NHS have allocated a paltry £6 million to treat 1000 obese children per year with a comprehensive pilot program. On the other hand, the cost of vaccinating all 12 million kids? £264 million in cash to Pfizer (that would account for just a single dose). That figure does not include the financial and human costs of adverse reactions. Would the money not be better spent on treating the obesity pandemic?
Intervention in childhood, before the children have developed diabetes, cardiovascular disease, cancer and other diseases associated with disrupted metabolism, would greatly improve quality of life for each and every child! When discussing this with my eight year old son he pointed out that “they get bullied,” so emotional harm needs to be considered as a risk factor of obesity as well.. Treating children for obesity now would further provide some inoculation against future pandemics.
We would simultaneously be cultivating resilience against future infections and reducing the burden of chronic disease on our healthcare system.
What about natural immunity?
Vaccination effectiveness wanes after 6 months. This means that we would have to vaccinate 5-11 year olds twice a year at that huge cost, and with many potential risks. Natural immunity to viruses generally last a lifetime, and is more effective in protection against new variants. Survivors in of the 1918 Influenza had strong natural immunity 90 years later in a study conducted in 2008. (https://pubmed.ncbi.nlm.nih.gov/18716625/). Adding to the case for natural immunity a study in Qatar has shown that severity of re-infection is vastly reduced compared to primary infection. Natural immunity reduced the chance of re-infection by over 85% and there was not a single case of severe infection or death. (https://www.nejm.org/doi/full/10.1056/NEJMc2108120?query=TOC). Vaccinating individuals with previous infection provides negligible added protection while dramatically increasing the risk of side-effects. (https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1.full).
Healthy food and lifestyle choices too, last a lifetime and apart from preventing severe outcomes when infected with Covid, have many additional benefits for mental and physical health.
Additionally there are evolutionary mechanisms by which vaccines can drive the evolution of new variants – this is logical: if the spike protein is what the vaccinated immune system recognises then the virus will evolve variants with different configurations of its spike protein – natural selection in action.
However, natural immunity responds to dozens of different viral antigens, thereby conferring greater protection. A herd of children with natural immunity will be less likely to be an evolutionary testing ground for new variants attempting to “escape” the vaccine.
By not putting selective pressure on viruses to escape vaccine induced immunity, we will help maintain effectiveness of the vaccines in high risk individuals.
Lastly, since we know that the vaccines are effective at preventing hospitalisation and death amongst vulnerable adults (keeping in mind that 95% of those that die have co-morbidities and an average age of 83,) AND we have a variety of effective treatments (including new drugs, old drugs such as Invermectin, vitamin D, Zinc, etc.), do we really need to be vaccinating children? I suggest that the risks are not worth the purported benefits. Furthermore, the financial and human resources could be used much more effectively to support other strategies that would have a benefit for COVID (reduced hospitalization and mortality) while also addressing other causes of suffering and illness and generally resulting in a better quality of life.
I’m writing to you to share my concern regarding the implementation of a COVID vaccine passport.
I will share both my personal and my professional perspective.
I’m a French/American living in Scotland since 2011, and am now settled in Ullapool. I am here because I love Scotland.
I graduated with High Honours in Biology from Oberlin and have a MS. in Herbal Medicine. I’ve been practicing as a herbalist since 2011 and am also a psychotherapist.
To start off I would like to step aside from the fundamentalist camps of “pro-vaccinators” and “anti-vaxxers.” As is so often the case such polarised black and white statements are rife with confirmation bias, cherry picking, misinformation, and false assumptions. Having lost the ability to compassionately listen to “the other” they have also lost the capacity for rational discourse.
Declaration of bias:
As a herbalist I work with clients with serious life-threatening and debilitating conditions. I have a strong preference for natural medicine and nutritional and lifestyle interventions. However, my strongest value is that my clients receive the best possible treatment. Some of my patients wish to forego treatment with drugs or surgery and I encourage them to consider an integrated approach. Others wish to go ahead with treatments that I deem unnecessary, ineffective, or even dangerous. It is my job to put aside my personal values (while being transparent about them), and to collaborate with the client to come up with the best possible strategy for addressing the clients condition in alignment with their needs and values even if I disagree. I am diligent in my research and contextualise it within my framework of herbal and functional medicine and strive to come up with the most effective recommendations for my client. I see vaccines as one tool amongst many that have a role in individual and public health.
So lets work from some basic assumptions. These assumptions can be questioned – they are evolving with the situation, with our medical knowledge, and with the virus. These are statements we can make now that are rational, reasonable, and have a foundation in the medical literature.
1 – The vaccines for COVID-19 are relatively effective. They do a very good job at reducing mortality in at risk individuals.
2 – The vaccines are relatively safe. They have a fairly small rate of adverse reactions. However, the adverse effects can be serious – life threatening or debilitating. Furthermore long-term side-effects have not been studied. A caveat needs to be made here. Adverse reactions are dramatically under-reported. I’ve seen studies that estimate that only 5-10% of adverse reactions are reported. So possibly one might multiple the stated number of adverse reports by 10-20 times. We are working with many unknowns.
3 – COVID is dangerous in people with risk factors. Mortality figures show that the vast majority of people who die with COVID have co-morbidities. I’ve seen one study showing that 95% of those who die with COVID had one or more co-morbidities. Sometimes people with no known risk factors also have a severe infection, but this is a statistically small number.
4 – The vaccine rollout in the UK has greatly reduced mortality. Those who are at risk have for the most part been vaccinated if they choose.
5 – Viruses evolve. Vaccines can be a driver for viral evolution. The virus will adapt to the vaccines.
6 – Natural immunity is more effective and longer lasting than vaccine protection.
7 – Asymptomatic transmission is exceedingly rare. Cases of outdoor transmission are even more rare.
8 – Vaccinated individuals can be infected and they can transmit the virus.
9 – Masks are effective at reducing transmission.
These are not facts but they all align with the current evidence. They provide a place to start when making a decision.
The vaccine passport is in my professional analysis, unwarranted on scientific grounds, and likely detrimental to individuals, businesses, and society as a whole.
As often is the case there is tension between individual health public health. This is made very clear in the challenge of making decisions in a situation such as an epidemic.
In the beginning stage of the epidemic it made sense to have broad sweeping measures, these allowed us to buy time as we learned about COVID, who was at risk, how to treat it, etc. But we are at a different stage now. A case can be made that we have successfully protected the vulnerable, that mortality rates have dropped, and that it is now time to stop counting infections. We don’t count flus or colds and humans and COVID need to enter into a long-term relationship. Vaccination will not achieve “herd immunity” but natural immunity will develop allowing humans and COVID to settle into a more “comfortable” relationship. Vaccines beyond the high-risk may actually interfere with this process.
As a practitioner of herbal medicine what catches my attention are the risk-factors. Many of them are treatable with dietary and lifestyle interventions. Virtually all of them are treatable with herbal medicine. The simplest one to address would be vitamin D. The research on Vitamin D is unequivocal and supplementation would reduce hospitalisation and mortality at a very low cost, with zero risk, and with many side-benefits as low vitamin D status is implicated in many health conditions. From the natural medicine perspective we are missing out on an opportunity to improve public health by tackling malnutrition, sugar consumption, obesity, diabetes, heart disease, etc. These are low cost interventions with sweeping benefits to the quality of life of all. I find it quite dissonant that healthy individuals would be pressured to take a vaccine while we wouldn’t dream of pressuring individuals with risk factors to lose weight, or change their diet, or even take a vitamin D supplement (which some studies show could reduce mortality by 80%).
On a psychological note I believe that top down approaches tend to increase resistance. If you want people to follow health guidelines coercing them with vaccine mandates and passports doesn’t promote a trust between the people and their government. If you want people to get stubborn and dig in their heels do something that is authoritarian in nature. It undermines the individual drive to make socially responsible decisions. It is overbearing and what many would deem “patriarchal.” It will negatively impact individual, communities, and businesses of all sorts. It forgets the vital role of trust and responsibility that must go both ways between citizens and their elected government. Such trust is a necessity for good governance. We need to trust that when given clear information individuals will make socially responsible decisions most of them time. We live in a complex world and what one person thinks is right may not be in agreement with what another may think or what the “majority” may think. This is what creates a diverse culture and species that is adaptable, that grows, and that is rich. Diversity is a requirement for survival – as we can see with viruses – its their diversity that allows them to adapt to interventions such as vaccines.
As a medical practitioner I have serious ethical concerns: I think that decisions for medical intervention needs to be made between the client and their practitioner. They are private and personal. Government officials are not trained in science, biology, immunology, medicine, statistical analysis, biochemistry, herbal medicine, etc. Trumping the sacred relationship between medical practitioner and patient is highly problematic. Furthermore coercing vaccines is a violation of an individual’s right to make choices regarding their body and well-being. If the vaccine were 100% effective, and 100% reduced transmission, and 100% safe and furthermore if the virus hit everybody unpredictably a case might be made for a vaccine mandate. However the situation is much more ambiguous. I’m grateful that the vaccine is effective in those who are vulnerable. This is the most important point. Going further is going too far. We know that vaccinated individuals can transmit and that asymptomatic transmission is rare. This largely disassembles the pseudo-logic behind the case for vaccine passports.
Though I do not find it so evident in the UK as in the US I find the scapegoating, name calling, blaming and shaming that is being directed at those who don’t want to vaccinate immature and reprehensible. It has no scientific basis and is rife with hypocrisy. We are not mandating that fat people lose weight (to speak in an equivalently rude fashion) though this might have a bigger impact on mortality than vaccinating low risk individuals. There are many ways of taking responsibility for one’s impact on the world and in this situation (maybe in any situation) there is no call for slandering or guilt-tripping others.
Living in Ullapool, I was impressed at how the community came together in its own way to address the epidemic. People organised to deliver meals to those who needed to isolate, funds were raised for those who could not work and yet were given no support from the Scottish government to even feed themselves. People took care of each other – it is a natural human impulse. It is such a coherent community based response that accepts individual contributions that must be celebrated and encouraged. Diversity of opinion is what creates adaptability and resilience. I feel confident that Ullapool can rise to the occasion of future challenges (like climate change) but I am in doubt when it comes to the over-arching response of the government. Vaccine pressure further reinforces my doubt and undermines my respect for political parties such as the SNP and the Greens with whom I share many values.
The decision to have vaccine passports doesn’t bring us one step closer to freedom but instead goes directly in the opposite direction – imposing limitations on a vast number of individuals in a way that is ethically untenable, logically and scientifically flawed, and politically oppressive. It will create division and anger, disfranchise many, place a burden on businesses (and musicians, roadies, sound engineers, etc) and create further rifts in the fabric of our society. We need to be able to gather and celebrate, this is a vital human need and a human right, and it needs to be facilitated. A reasonable case can be made for temporary measures such as a combination of masks, ventilation, number restrictions and maybe even free COVID tests but in the long-run we need to return to a free and open society.